









View Featured Categories
What We Know and Don’t Know About the Vaccine and Virus





The largest human experiment in history isn’t over yet.
Spike protein, whether from SarsCoV-2 infection or the MRNA vaccine has left the public and scientific community with a lot of questions. These vaccines were used in 94% of people who took the covid vaccine in the United States.
How does the SarsCoV-2 virus infect the body?
SARS-CoV-2 is an enveloped virus, meaning that it has a lipid membrane (an outer covering made of a fat-like substance). The protein spikes covering the virus's envelope allow it to bind to receptors on the host cell's lipid membrane (via ACE2 receptors), leading to infection.
What about ACE2 receptors? How are they involved?
ACE2 receptors are found throughout the body but are especially in intestinal epithelial cells of the gut, endothelial and smooth cells of the blood vessels, heart (epicardia, adipocytes, fibroblasts, myocytes, coronary arteries), brain, testis, and on tubular epithelial cells of kidney. The SARS-CoV-2 present as droplets in the air enters the upper respiratory tract, affecting the nasal and pharyngeal epithelia of a healthy individual the infection proceeds into the lower respiratory tract, and infects bronchial and alveolar epithelium, causing symptoms of cough and fever.
The virus soon enters the peripheral bloodstream through the lungs and develops viremia (when the virus enters bloodstream). Here, the ACE2 receptors serve as the gateway for the entry of the virus inside the body.
The virus replicates and simultaneously hampers other organs expressing ACE2, such as the heart, kidneys, blood vessels, and gastrointestinal tract. The massive epithelial and endothelial cell death and vascular leakage trigger the production of inflammatory cytokines and chemokines.
Hijacking of pulmonary ACE2 receptors, their downregulation, and shedding causes dysfunction, inflammation, and vascular permeability, this might be the possible cause behind the acute lung injury. The fast-approaching cytokine storm further hinders the immune response and causes dysfunction. (1)
How does the vaccine mRNA work and how is it different than traditional vaccines?
Traditional vaccines work by giving a person either viral proteins or an inactivated or weakened version of a virus that triggers an immune response. mRNA vaccines do not contain viral material. Instead, these vaccines contain lipid or fat bubbles that surround a segment of mRNA, which provide cells with the instructions to make a certain viral protein.1) (About genomics fact sheets, 2021)
What is the difference between the SarsCoV-2 virus and the mRNA vaccine?
According to Dr Peter McCullough on Courageous Discourse: “ ‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA”
- Parry, et al, published a comprehensive review on the litany of Spike-protein diseases that occur after its widespread distribution in the body. Here are some of their evidence-based teaching points:
- SARS-CoV-2 spike protein is pathogenic, whether from the virus or created from genetic code in mRNA and adenovector DNA vaccines.
- Biodistribution rodent study data show lipid nanoparticles carry mRNA to all organs and cross blood-brain and blood-placenta barriers. Some of these tissues are likely to be impervious to viral infection; therefore, the biohazard is particularly from vaccination.
- Lipid-nanoparticles have inflammatory properties.
- The modification of mRNA with N1-methylpseudouridine for increased stability leads to the production of spike proteins for months. It is uncertain how many cells and from which organs mRNA spike proteins are produced, and therefore, the exact effective dose delivered per vaccine vial is unknown.
- The long-term fate of mRNA within cells is currently unknown.
- The mRNA and adenovector DNA vaccines act as “synthetic viruses”.
- In the young and healthy, and even in many older individuals with vulnerable comorbidities, the encoding-based COVID-19 vaccines will likely transfect a far more diverse set of tissues than infection by the virus itself.
- Evidence suggests reverse transcription of mRNA into a DNA copy is possible. This further suggests the possibility of intergenerational transmission if germline cells incorporate the DNA copy into the host genome.
- Production of foreign proteins such as spike protein on cell surfaces can induce autoimmune responses and tissue damage. This has profoundly negative implications for any future mRNA-based drug or vaccine.
- The spike protein exerts its pathophysiological effects (“spikeopathy”) via several mechanisms that lead to inflammation, thrombogenesis, and endotheliitis-related tissue damage, and prion-related dysregulation. Interaction of the vaccine-encoded spike protein with ACE2, P53, and BRCA1 suggests a wide range of possible biological interference with oncological potential.
- Adverse event data from official pharmacovigilance databases, and an FDA-Pfizer report obtained via FOI, show high rates and multiple organ systems affected: primarily neurological, cardiovascular, and reproductive.
- Pfizer and Moderna mRNA COVID-19 vaccines’ clinical trial data independently interpreted has been peer-reviewed and published to show an unfavorable risk/benefit, especially in the non-elderly. The risks for children clearly outweigh the benefits.
- Repeated COVID-19 vaccine booster doses appear to induce tolerance and may contribute to recurrent COVID-19 infection and ‘long COVID’.
In other words:
- Whether from virus or vaccine, COVID is pathogenic (originating or causing disease).
- The lipid nanoparticles that are in the vaccine are inflammatory, cross the blood-brain barrier and placental barrier, can enter all organs, and are potentially more harmful than the viral infection.
- Production of spike proteins from the vaccination can last for months. No one really knows how long; speculation is they could last for years.
- There is evidence that the mRNA vaccine can enter DNA through a process called reverse transcription. This means that the mRNA could be found across many generations.
- The vaccine exerts its effects and is expressed in many ways, potentially causing harm in the cardiac, respiratory, and gastrointestinal systems, along with causing or exacerbating autoimmune conditions and causing tumors. This statement is backed up by a freedom of information request: An FDA-Pfizer report obtained via FOI, shows high rates and multiple organ systems affected: primarily neurological, cardiovascular, and reproductive.
- Peer-reviewed and published data show an unfavorable risk/benefit, especially in younger age sets, especially true for children.
- Repeated COVID-19 vaccine boosters appear to lead to induce tolerance and may contribute to recurrent COVID-19 infection and ‘long COVID’.
And probably the most frustrating part of it all is we really do not know how long the vaccine lasts in our bodies.
Nature to the Rescue
Nattokinase (2,3) is the foundation to detoxify naturally.
There have been many drugs attempting to reduce and dissolve the spike protein, thereby rendering it useless. The answer may be found in over-the-counter substances found in nature.
Nature's profound ability to dissolve spike proteins, downregulate inflammation, and restore and repair injured tissue is nothing less than amazing. Dr. Mccullough has developed a protocol to help the body detoxify from both the vaccine and those suffering “long COVID” and other pathologies.
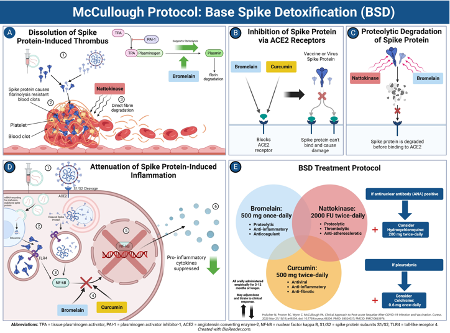
McCullough Protocol Base Spike Detoxification

- Dissolution of spike protein-induced thrombus. Nattokinase directly degrades fibrinolysis-resistant fibrin from the spike protein, and bromeliad upregulates fibrinolysis
- Inhibition of spike protein via ace 2 receptors. Bromelain and curcumin block the A 2 receptor preventing spike protein from binding.
- Proteolytic degradation of spike protein. Nattokinase degrades spike proteins, rendering them inactive.
- Attenuation of spike protein-induced inflammation bromelain curcumin down regulate the signaling pathway induced by spike protein leading to the suppression of inflammatory molecules. (4)
Citations
- Shirbhate E, Pandey J, Patel VK, Kamal M, Jawaid T, Gorain B, Kesharwani P, Rajak H. Understanding the role of ACE-2 receptor in pathogenesis of COVID-19 disease: a potential approach for therapeutic intervention. Pharmacol Rep. 2021 Dec;73(6):1539-1550. doi: 10.1007/s43440-021-00303-6. Epub 2021 Jun 27. PMID: 34176080; PMCID: PMC8236094.
- Tanikawa T, Kiba Y, Yu J, Hsu K, Chen S, Ishii A, Yokogawa T, Suzuki R, Inoue Y, Kitamura M. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405. doi: 10.3390/molecules27175405. PMID: 36080170; PMCID: PMC9458005.
- Weng Y, Yao J, Sparks S, Wang KY. Nattokinase: An Oral Antithrombotic Agent for the Prevention of Cardiovascular Disease. International Journal of Molecular Sciences. 2017; 18(3):523. https://doi.org/10.3390/ijms18030523
- https://www.jpands.org/vol28no3/mccullough.pdf?ref=BRAND
Written by Brooke Lounsbury




